The Health
Ombudsman has taken up the case of the sexual
assault on a patient who had her knickers removed
during an operation by a nurse even after she
had expressly forbidden it and she was then given a
suppository against her consent. The hospital have
constantly refused to investigate the case and
discipline the staff and interestingly when the GMC
investigated no one would admit removing the patient
knickers or giving the suppository or seeing anyone
do it. If it was done as a genuine mistake one would
expect people to own up and say SORRY.
Due to the work
load it will be 7 months before the Ombudsman can
start their investigation. In the mean time will
a nurse and the other nurse continue to sexually
assault more patients? The Ombudsman has found in
favour in this case once and passed it back to the
HCC who said a doctor can force treatment on a
patient if its in their interest even if they say
no. This is of coarse a stupid statement against all
British law and it seems the HCC were upset as the
Ombudsman found they hadn’t done their job properly,
they did fight it and it had to go to the highest
level in the Ombudsman .
Leighton Hospital TOLD TO IMPROVE
09:56 - 09 October 2007
The organisations running the ambulance service and
Leighton Hospital
have been told to improve how they handle
complaints.
An audit carried out by the Healthcare Commission
has revealed that
North West Ambulance Service (NWAS) NHS Trust and
Mid Cheshire Hospitals
NHS Trust are not meeting the basic standard to
ensure patients,
their relatives and carers are not discriminated
against when complaints are made.
The audit also revealed that NWAS Trust's complaint
system needed
to be more accessible in terms of registering formal
complaints
and feedback on the quality of services.
The healthcare watchdog launched the audit after
becoming concerned
about how patients' complaints are handled locally.
The trusts were two of 32 chosen for inspection
because of concerns
that they were not meeting Government standards.
The basic standard requires trusts to make complaint
procedures
accessible, ensure complainants are not
discriminated against
and act on concerns and make changes where
appropriate.
The Healthcare Commission said that trusts should do
more to
make it easier for people to raise a complaint.
Mid Cheshire Hospitals NHS Trust, which runs
Leighton Hospital,
received 288 complaints in 2006/7 - a drop on the
previous year's
figures of 300 - and has received 147 complaints
this year to date.
Officials reacted to the Healthcare Commission's
findings by
forming Matron Forums for staff to discuss complaint
handling.
A spokesman said: "A thorough audit of complaints
has taken place and
systems have been implemented to ensure staff are
trained in dealing
with complaints."A NWAS spokesman said: "North West
Ambulance Service
NHS Trust treats complaints very seriously and
welcomes the findings
of the audit to ensure best practice is achieved
across all areas.
"Following the audit on complaints handling within
the former Mersey
Regional Ambulance Service NHS Trust, areas for
improvement were noted
by NWAS and included in the trust's action plan.
"NWAS immediately reviewed and amended its new
complaints policy and
stated its intention to provide information on staff
attitudes, staff
support and emphasised the issue of not
discriminating against
complainants of the services it provides.
"The Healthcare Commission acknowledged the swift
action
the trust has taken in response to the findings.
"The trust remains committed to ensuring all its
staff
are fully aware of the trust's complaints policy and
procedures."
Have you lodged a complaint with one of the trusts?
Trust fined £14,000 for Leighton hospital patient’s fall
MID Cheshire Hospitals NHS Trust has been fined £14,000 after a man
with mental health problems was seriously injured in a fall from a
window at Leighton Hospital in Crewe. The patient, a 30-year-old who
has not been named, was injured in the incident when he managed to
climb out of a first-floor window at the hospital on August 4, 2005.
The Trust, which manages Leighton hospital, was fined £12,000 for breaching
the Health and Safety at Work Act, £2,000 for breaching health and
safety management regulations, and was ordered to pay £3,982 costs
at a hearing at Crewe Magistrates Court.
A Health and Safety Executive spokesman said the hospital had failed
to learn from similar incidents in the past or take on board
guidelines issued by the NHS, and urged bosses at Leighton hospital to take
action to ensure the same cannot happen again.
AN ELDERLY woman was kept waiting for a sight-saving operation in a
hospital waiting room for four hours – then sent home because her
medical files had gone missing.
Seventy-four-year-old Ivy Long was due to have cataracts removed
from both eyes on Thursday, but must now spend another two weeks
with blurred vision.
Ivy, of Queensway, Winsford, had had nothing but a glass of water
from 7am when she arrived at Leighton Hospital at 11.45am. Her
husband, Jim, had an angina attack at the hospital due to the stress
the mix-up caused.
‘In today’s age of computers you would think they’d be a bit more
organised,’ said Jim. ‘It’s not good enough.
Leighton Hospital
If you have been
abused or sexually assaulted by Health Care workers the site above
may be able to help
From
the Post Bag
I must bring to your attention the disgusting state of the
"Chapel" of rest at Leighton Hospital. My niece died on
Monday morning on Ward 7 and was moved to the chapel for
visiting at Lunchtime.
Unfortunately this experience totally undermined all the
skilful nursing care that my niece received on ward 7. The
trolley was completely viewable from the viewing window as
was the mattress. My niece was draped in an unironed sheet.
This part of the hospital was more like a spoof scene from a
Carry On film. Thank God my elderly parents decided they
were unable to make this visit, they would have been
appalled and horrified.
This area needs to receive urgent attention, a most
unsatisfactory experience in 2008 and a disgrace on Leighton
Hospital and the trust.
Sean T Traynor
Sean T Traynor
The Fox
Inn
Troston Road
Honington
Bury St Edmunds
Suffolk
IP31 1RD
S West
went into hospital 2007.
I was interested to read your campaign against sexual
abuse as the very same thing happened to me. I went into
Leighton Hospital for a leg operation and went into surgery
with my underwear on when I came out of surgery I had had my
knickers removed without my consent and I felt sexually
violated. The operation site didn't require my knickers to
be removed so why did they do it. The thought of a
group of people removing my knickers and seeing all my
private parts when I was unconscious and unable to defend my
self makes me sick. If this had happened anywhere else the
people that did it would be up before the courts for sexual
assault. The hospital doesn't seem to have any idea of
patients feelings you are just a piece of meat the other
worrying thing is if any of the people who do this are
perverts in any way they are getting away with it with no
check on them. Procedures must be put into place to protect
patients so that no one can have their underwear removed
without written consent unless its an emergency.
J
Jones (Went as a patient) said on
29 Jan 2008
Staffing levels seemed to be inadequate. On one night shift
there were only 2 nurses covering 3 wards which contained a
large proportion of people confined to their beds. On this and
many other occasions people were ignored when they pressed their
call buttons. I personally, and others in the ward, waited
regularly from between 5 and 20 minutes for a bed pan and even
when we got one we were often left perching on them for similar
time periods. This was very distressing for some patients, and I
found it very difficult as I was in a lot of pain from a broken
hip. I personally dread having to come back into hospital for
any length of time if I have to go through the same experience.
When I was in hospital for a week prior to my recent stay I
witnessed similar levels of care with many elderly patients not
receiving the care they deserved and often being ignored.
I also think some staff should consider patients feelings during
shift hand over. I was talked about as if I was stupid, some of
the facts were incorrect at hand over and some of the nurses
seem to think you are deaf and can't hear what they are saying!
I was upset by some of the tactless comments made at hand over.
Communication overall could be improved.
Webmaster Note it seem
that Leighton Hospital hasn't changed in its care of the elderly
since the HCC report and its frightening
that people are still treated this way in 2008 if you are
old and need to go into hospital you can choose which one you go
into you should read the HCC report and these pages and then
make an informed decision which is the best hospital for you
Anonymous 1 (Went as a patient)
said on 17 Dec 2007
What you liked:
The midwifery staff in general were friendly, however there was
a great variation of staff who appeared unprofessional and
uninterested to the wonderful but few, who were brilliant and
trying to pull the weight of all the staff who really couldn't
be bothered.
Morale appeared very low.
What could be improved:
My labour was difficult with the midwife delivering my baby
pronouncing that she wasn't very good at this! Praise God for a
senior midwife stepping in and taking over.
Staffing levels were very poor, my baby was supposed to have
hourly observations, however this was only done once!
I have a medical condition which means it is very hard for me to
get around, when i arrived on the ward the midwife was brilliant
and very helpful, however once the shift changed i didn't see
anyone till i hobbled down to the desk to ask for help!
The hospital was dirty with blood on the floors and in the
bathrooms and dry vomit on the frame of the bed!
The discharge process was very poorly organised and despite
having been seen and discharged by the doctors it took the
midwifery staff several hours to fill in the tick chart for our
discharge.
Fury at patients left
malnourished
Feb 6 2008
HUNDREDS of patients have been discharged malnourished from
Leighton Hospital, according to shock figures discovered by an
MP.
Tory Stephen O’Brien, whose Eddisbury constituency covers the
Crewe hospital, found from 2006-07, 842 patients left
malnourished from Leighton and the Victoria Infirmary, Northwich,
which are both run by the Mid-Cheshire Hospitals Trust.
The Shadow Health Minister says the Government’s own figures
show across Britain, 139,127 patients were discharged from
hospital malnourished – an 84% increase on 1997-98.
A total of 130,594 patients were admitted to hospitals in a
malnourished condition – an 85% rise from 1997-98.
Mr O’Brien said: “It is a scandal that in 21st Century Britain,
we allow vulnerable patients to be let out of hospital in a
malnourished state, and it is even worse that we allow thousands
of patients to get more poorly while they are in hospital.
“Malnourished patients are more prone to infections, have more
complications after surgery, and have higher mortality rates –
yet the Government allows over 130,000 patients to enter
hospital in that state.
“Nurses need to be given the time and equipment to get on with
the job of caring for our most vulnerable patients.”
A spokesman for the Mid-Cheshire Hospitals Trust said it had
introduced a number of initiatives during the past few years
which aim to ensure the nutritional and dietary needs of
patients are fully met during their stay at either Leighton
Hospital or Northwich Infirmary.
“All patients identified with malnutrition are referred to a
named ward dietitian and seen within 24 working hours, These
patients are given a care plan, and where required, assistance
at meal times.”
Emma Whittle, senior dietitian at the trust said: “Good
nutrition is an essential element in patient care and recovery,
so it is important patients are encouraged to eat and drink with
the assistance of nursing staff, a family member or a volunteer
mealtime assistant.
“In some instances, the help given may be as simple as
unwrapping a bread roll or cutting up food for the patient to
feed themselves. However, a considerable number of patients
benefit from having one-to-one encouragement and assistance with
their meal.
“When patients leave hospital, many may still be classed as
‘malnourished’’ but they will be receiving intensive treatment.
Malnutrition is not something that can be rapidly corrected.”
A&E Leighton Hospital
I attended Leighton Hospitals A&E with a
patient who had a suspected broken leg knee. After a 2 hour weight
we saw the doctor who asked the patient to jump up on the bed. The
patient was crying as it was with pain sitting in a wheel chair.
When I pointed out the fact the patient was small and couldn’t jump
up on the bed if she was fit the doctor said I am not bending down
to look at the knee. The patient was then crying with extreme pain
forced to try and climb up on the bed. If the leg was broken it
could have pushed the bone through the skin.
After xray it was decided that it was badly
strained and swollen. The doctor offer the crying patient pain
relief and asked are you allergic to anything who replied yes
Paracetamol and it will be on my notes.
The patient was then given tablet containing
Paracetamol which if she had taken could have been fatal even a
child would not have given these tablets knowing she was allergic.
Webmaster Note Is the Doctor that gave
the Paracetamol totally incompetent or was this a
deliberate act as this patient has a complaint against the
hospital. If this was the case then its a very serious case but
its hard to see why when she was told of the allergy and its on
the notes she still gave what could be a fatal medicine.
Some of the
questions and the answers from the Health Commission Survey of
patients. To get a full picture you must read all the surveys
at the link above. We have picked on these answers as they show that
by the HCC survey that a lot of people are not giving
informed consent to treatment and the answers for side effects
is very low all round. If informed consent isn't given then consent
is invalid.
Question
Leighton
Best NHS
Did staff explain why any tests were needed?
79
89
Did staff tell you how you would find out the results of
tests?
75
89
Did staff explain the results of tests?
68
82
Did staff explain what would happen before any treatment?
88
95
Did staff explain the risks/benefits before any treatment?
82
91
Did staff tell you about medication side effects?
53
75
This site is run to fight for justice and
freedom and protect the weak. The information on this site is collected
from a variety of sources Government Depts , Press, Newsgroups, BBC,
Medical forums and anonymous members of the public. The site is
hosted outside of the UK in various locations across the world. As
such its contents can’t be affected by any UK court or court order
and any attempt to have the site removed by UK courts will fail. The
owners of the site will not reveal any of the contributor’s names to
any UK court and indeed may not even know them anyway see our
main page.
The only way to shut this site down is for
Leighton Hospital to stop making mistakes that ruin people’s lives. Once this has been achieved
the site will no longer be needed. It provides a voice for these people so that
they can be heard without threats of legal action from the hospital.
We have been under attack by lawyers
working for Leighton Hospital who have attempted to take this
site and other sites down this has been done by issuing threats
contacting ISPs and threatening victims whose stories are
mentioned on these sites. Their attempts have failed and if the
site should be ever shut down then 50 new ones will appear all
over the world within hours and I have told them this. If
Leighton Hospital spent more money on patients and less on fancy
lawyers this site wouldn't be needed.
We find it frightening that Leighton hospital
should go to such lengths to hide the truth it makes us believe
that there is more going on than was first thought and that they
are trying to cover some great mistake. Due to this attack we
have stepped up our efforts to discover what they are hiding. We
are seeking information and if you have any knowledge of the
following please get in touch.
The death of an old lady in November 11th
2005 in ward 11
The hospital giving out medical records
without the patients consent and these records being sent abroad
without consent.
Anyone who has been give a suppository or
had underwear removed without consent.
Webmasters Notes
This case has shaken the Hospital to the
extent that they have employed high power lawyers to harass
the patient and family who are witness in a GMC case and
they have attempted to have my sites removed by threats to
ISP's all of which have failed and resulted in me putting
more sites up all over the world.
Leighton Hospital have in
this case totally failed in there duty of care in this case.
The failed to obtain
informed consent as the GMC have identified that the doctor
taking the consent couldn't give enough information for
informed consent so technically the whole operation was
assault.
The failed to assess her
anaesthetic needs which resulted in her nearly dyeing and
being in extreme pain.
The gave 10 mg of
Midazolam in one dose as shown on her records which is
potentially fatal.
They gave 900mg of local
instead of 400mg and didn't give adrenaline which was nearly
fatal.
She was sexually abused by
having her knickers removed when she had expressly forbidden
it.
She was sexually abused by
them giving a suppository when she had said no.
They failed to take care
of her pain relief.
What is worse when they
complained they failed to find anything wrong and cover up
what had happened. After the GMC HCC and Ombudsman have
found all the problems its hard to see why Leighton Hospital
didn't find anything wrong but put further patients at risk
from the surgeon another potental Barbara Salisbury. They
are refusing to name the nurses who sexually assaulted this
patient Witness are helping to fight this case
and the people who did this will be brought to justice.
My partner went into Leighton Hospital Crewe for a very
simple hernia operation to be done under local anaesthetic
and sedation she was supposed to go in at 12 and be home for
2 oclock the operation was supposed to last 30mins.
She gave consent for sedation and local anaesthetic but this
was not INFORMED consent as at no time did they tell her she
would be in terrible pain or may die from the sedation, or
that no anaesthetist would be present. The GMC in there
investigation found that the young doctor who took the
consent didn’t have the knowledge to answer any question or
give enough information for the consent to be valid the
hospital in one of their reply state She was given
insufficient information about the operation Therefore the
whole operation was done without consent which makes all
those who took part guilty of Assault and battery
The operation was carried out on November 11th 2005 at
approximately 3pm.We arrived early as requested at 11:30 and
went to the new medical centre at which point I was told
that the patient must go in alone as partners weren’t
allowed. She sat there alone terrified from 11:30 until 3
oclock and during this time a nurse asked her how she would
pay for her pain relief. She was shocked as she was told not
to bring valuables into the hospital. The nurse said if she
wanted pain relief after the operation she would have to pay
for them.
Before the operation when they were preparing her she told
the sister she didn’t want her knickers removing and the
sister agreed she could keep them on as they were not in the
way she also told the Doctor she didn’t want a suppository
for pain relief after the operation.
She was taken in for the operation and according to her
medical records given 10 mg of Midazolam in one go which is
a potentially fatal dose. The hospital now deny their own
records and say it was given over a long period of time but
the evidence shows they couldn’t have done as the correct
dose is 1 mg over 2 mins and then wait 2 mins before giving
anymore total time 40 mins she was in theatre 10 mins after
the anaesthetist came and they state the surgeon gave the
sedation so unless he operated with one hand he gave all 10
mg in one go. Why the anaesthetist didn’t give the sedation
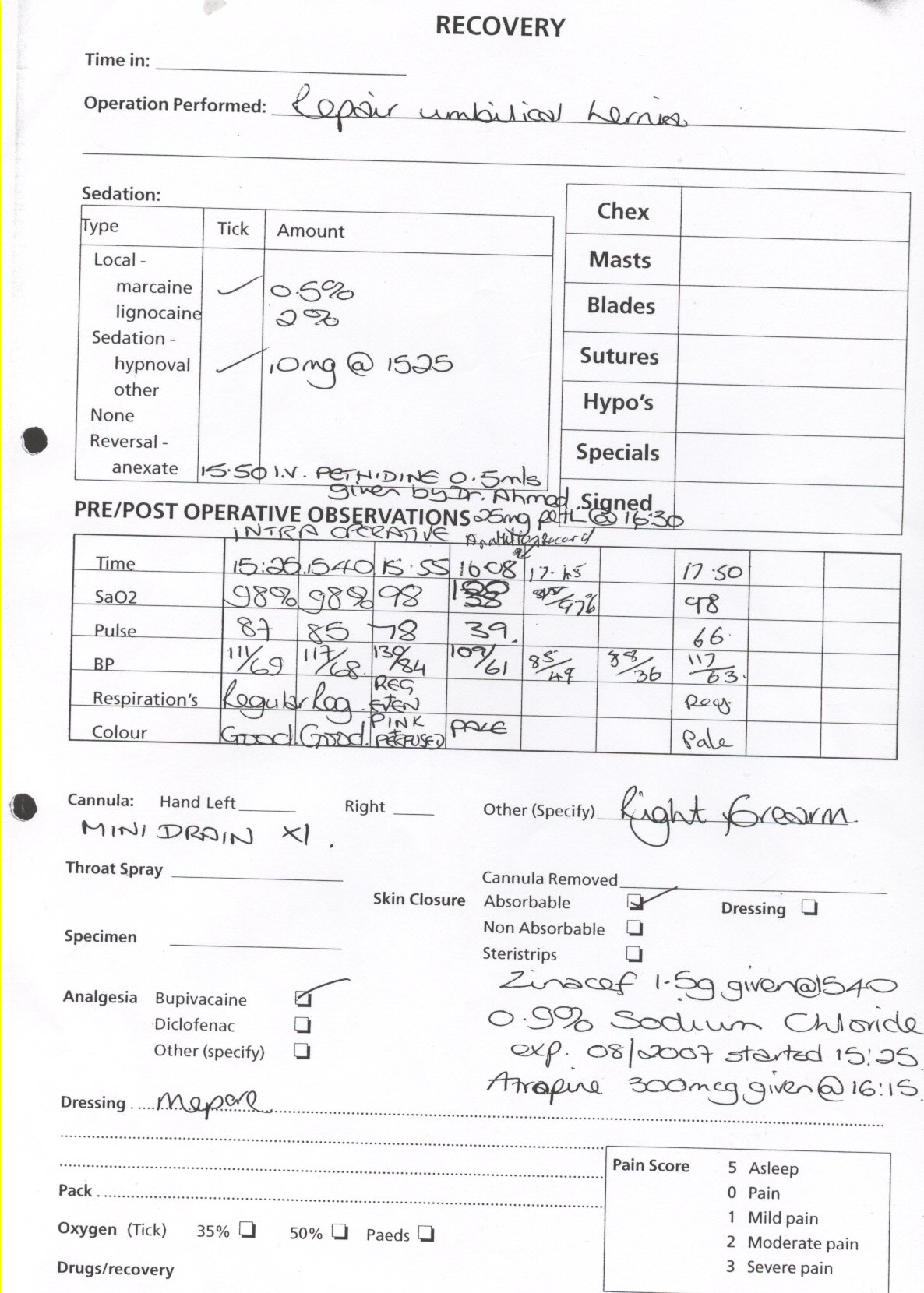
while she was there is a mystery. The operation chart
clearly show that she was given 10 mg of Midazolam in one go.
Midazolam is an interesting drug as its main use is to make
you forget what has happened to you and is often used to
take out teeth and other short term pain full minor
operations. Its not pain relief but can be used to make you
forget what happened so you don’t remember the pain and this
is often the case as its used as a cover up. If this
operation had only lasted 30 mins as it should we would have
never known what happened.
There is a lot of complaints about the use of this drug as
you forget what has happened but your subconscious mind can
still react to what happened see
http://ideas.4brad.com/archives/000100.html. It is also used
as a date rape drug and this means you cant remember being
raped but your mind will react to what has happened. This
makes things worse as you don’t know why you are having
strange feelings.
Its often used as a
Date Rape
drug and a male nurse got 7 years for using it
Midazolam
can lead to the patient experiencing daydreams with a
sexual content.
For more info see
Leighton hospitals own chart show she was given 10 mg midazolam in
one go but they now deny this. But look at the states for
15:08 its shows her O/2 level was down to 38% but someone
has changed it to read 100%. At no other time during the
operation was her O/2 ever 100% we believe this is a
deliberate forgery to hide what has happened. Note also how
they take the states every 15 mins but suddenly after her
heart drops they don’t take it again for over and hour other
information which they collected up to that point suddenly
isn’t recorded either. The surgeon Professor Aluwihare now claims he didn’t give
the sedation but left it to a very junior doctor who was
incapable of giving the drug properly but we have a letter
from Leighton Hospital solicitor stating that he did
administer the drug.
She was given local aesthetic for which according the Health
Care Commission (they investigate complaints about hospital)
the MAXIMUIM dose for her is 400mg which must be mixed with
adrenaline so the heart doesn’t stop they gave her 900mg and
no adrenaline. We believe this was negligence on their part
which could have killed her.
As soon as she was asleep they removed her knickers in the
most vile and perverted way without her consent even though
she had forbidden them to do so we believe this assault and
battery. This was done at the beginning of the operation but
the surgeon claims it was at the end so they could give the
suppository which the patient was awake and positive they
had already been removed so why do they lie? The nurse said
they were removed for none medical reasons ie to stop them
being stained with iodine.
She was asleep for the start of the operation but later when
she woke up during the operation and screamed with pain
which was 10 times worse than having a baby this is
everyone’s worse nightmare. She describes seeing all her
stomach covered with blood and her insides on her stomach.
They then suddenly realized she was awake and put a board up
so she couldn’t see. The surgeon claims he didn’t hear her
scream but was aware of her pain and her crying. The surgeon
called for an anaesthetist but there wasn’t any so he
carried on with her in pain he made no attempt to stop or
see the patient was all right. On 3 separate occasion she was
screaming the place down in pain and trying to get the mask
off as she shouted stop.
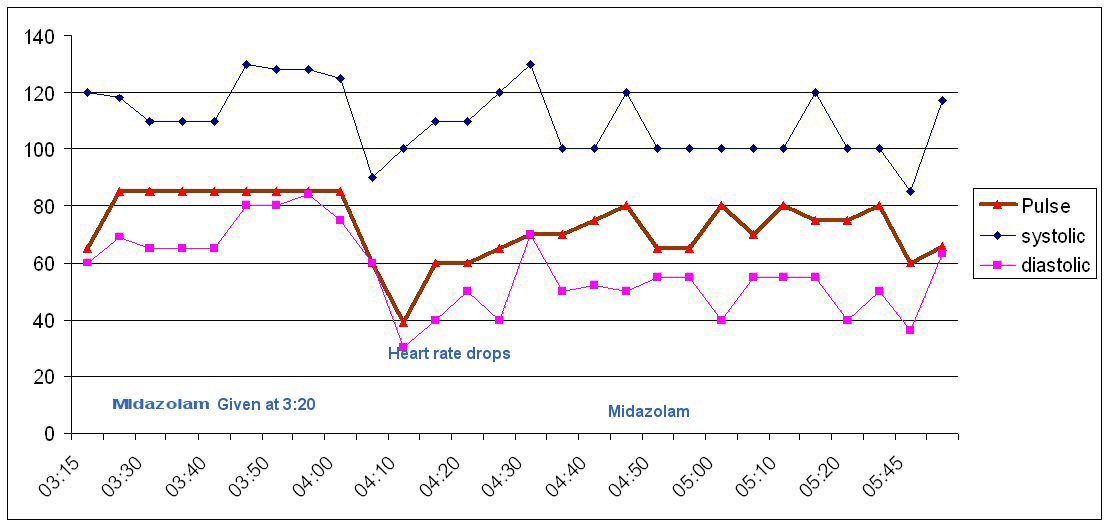
After 50 mins her heart rate dropped over 10 mins from over
80 bpm to 30 bpm at which point she passed out and believed
she died. She remembers the doctors panicking at this point.
She tried to tell them she couldn’t breath but she was
fighting for her life and unable to speak or get her breath.
It took them the ten full mins before they gave her a drug
to bring her heart back up. The chart shows what happened.
Click on the chart to see it full screen
An overdose of local or sedation can cause the heart to stop
and we believe this is what happened due to their negligence
this experience is life changing.
The operation finished after 2 hours and they then gave her
the suppository without her consent they simply lifted her
legs and said you have got to have this no explanation or
request she was still groggy from the sedation but knows her
knickers weren’t removed at this point as the surgeon
suggested. A similar case
http://www.bmj.com/cgi/content/full/310/6971/43 an
anaesthetist was struck off for the same thing.
She was kept in Leighton hospital for 2 days without any explanation
as to why and wasn’t told what had gone wrong or why the 30
min operation took over 2 hours. They kept saying she
couldn’t go home until a doctor had seen her but none came
we had to effectively force the issue by saying she was
going home now. While she was in Ward 11 she was terrified
as it was full of dieing people and in a statement to the
GMC's solicitors she describes how an old women was dieing
and kept asking for the nurses to call her family she was
told to shut up and go back to sleep and received no medical
treatment this went on all night. In the morning she had
died
We complained to the hospital the same day and made a formal
complaint within days of the operation and also the GMC and
the Health Commission who have taken a year to investigate.
Extract from the GMC Report
The surgeon Professor Aluwihare if you have any complaints about this man let us
know as the GMC would like to know
The GMC have filed a series of charges against the surgeon
Professor Aluwihare who did a runner abroad as soon as they investigated.
The Case Examiners have noted the
conclusions of the HCC report into this matter. It is
obvious that the HCC expert interpreted many of the facts of
the case in a way different to that of the experts
commissioned by the GMC. However, this may be explained by
the remit of the HCC being different from that of the GMC.
Both experts are united in the conclusion
that Professor Aluwihare should have seen the patient himself
earlier, and should have postponed the surgery if no
anaesthetist was available.
Professor Aluwihare either did not discuss
the procedure with the patient when he met her, or if he
did, failed to record what was discussed. Neither scenario
is good medical practice. Professor Aluwihare says he had a
detailed discussion but that he omitted to make a record. He
had delegated consent taking to Dr Ahmed, but did not ensure
that the patient was fully advised of possible risks
and complications. The expert's view is that a junior doctor
would be unlikely to be able to give detailed advice about
what an experienced surgeon would deem to be a difficult
operation.
Professor Aluwihare admits that the sedation
and supplemental pain killer was given under his guidance by
the House Officer. He disputes how much was given, believing
that the midazolam was not given as a 10 mg bolus, but in
increments, as recommended. The case notes would suggest
this is not the case as it is clearly recorded that 10 mg
midazolam was given at 15:26. It is in dispute whether 10 mg
bolus was an incorrect choice in the case of a patient as
large as the patent. However, as Dr Ahmed was acting under
direct instruction from Professor Aluwihare, it would appear
that the Professor had delegated the performance of the
sedation to someone who did not have the appropriate
competence and experience. Professor Aluwihare maintains
that midazolam was given incrementally. The midazolam,
therefore, was either given as a 10mg bolus, (which
Professor Aluwihare accepts would have been inappropriate),
or he failed to ensure that an accurate record was kept to
show that the drug was given in increments.
The expert opinions both believe that
express consent is required for the use of suppositories,
and that Professor Aluwihare did not obtain this.
The case is now referred to a Fitness to
practice panel
Leighton hospitals replied to our complaints
Main points from the hospitals replies
Dr R Okell, Clinical Director Anaesthesia has answered these
questions
Had the patient been given a general anaesthetic, she would
have certainly experienced less pain but as I advised you in
my previous letter, this carried a greater risk to the
patient because of her weight. Professor Aluwihare did ask
for an anaesthetist during the procedure but none was
available although one was present at the beginning of the
procedure and helped to get the line in. If one had been
available, they may have been able to increase the
efficiency of the sedation, which would have reduced the
likelihood of the vasovagal episode and the fluctuation in
pulse and BP might have been less.
Dr Okell tells me that he does not know how surgeons acquire
training in the use of Midazolam ( I find this reply very
frightening shouldn’t they know if people are qualified)
The patient says during the operation she was in so much
pain she was screaming the place down and crying. You ask if
we can confirm that she was screaming and for how long.
Professor Aluwihare tells me that he cannot remember The
patient screaming at all. She had discomfort from time to
time and articulated this quietly or briefly cried very
quietly. He tells me he could see The patient face and was
very aware of the need to control her pain.
Main points from the Health Commission
reply
The independent clinical adviser comments that it was
predictable that this would probably be a difficult and long
operation. A general anaesthetic was not contraindicated due
to the high BMI of 54, but would present significant risks.
However, the technique using local anaesthetic reduced the
risks of general anaesthetic, but carried risks associated
with local anaesthesia. The independent clinical adviser
clarified that the clinical records showed the amount of
local anaesthetic used was lidocaine (2%) 400mg, marcain
(0.5%) 100mg and lidocain (0.5%) 400mg.
In the clinical adviser’s opinion the maximum amount of
plain local anaesthetic would have been in the order of 3 x
138 (weight of patient) = 414mg. He states that it is
surprising that so much local anaesthetic was used and that
adrenaline was not added.
The patient was therefore possibly at risk from the dose of
local anaesthetic. However, having an anaesthetist present
would have reduced the risks as the anaesthetist would have
been able to monitor, administer appropriate drugs, and
resuscitate in the event of vomiting and aspiration which
was essential in such a patient (with a BMI of 54 and weight
138kg).
The clinical adviser recommends that the trust formulate a
policy concerning the presence of an anaesthetist,
especially when a patient receives large doses of local
anaesthetic, for abdominal procedures and patients with a
BMI of 54.
My expectation is that Mid Cheshire hospitals NHS Trust will
contact you in writing within the next 25 working days in
order to set out the steps that it will be taking in
response to the recommendations for further action that I
have made. I would also expect you to be informed in due
course of the outcome of that action, and I will be asking
the trust to copy the Healthcare Commission in on the
relevant correspondence. The letter was sent on 21 December
but the hospital has not complied with the above order in
the time stipulated.
The Ombudsman's report
The
Ombudsman has completed their investigation and found the
HCC failed to identify that the removal of a women's
knickers after she had said they couldn't be removed and
giving a suppository without consent must be reinvestigated
as soon as possible. We believe that this will reveal
that the patient suffered assault and battery which is a
criminal offence.
Battery is defined
A battery
is the wilful or intentional touching of a person against
that person’s will by another person, or by an object or
substance put in motion by that other person. Please note
that an offensive touching can constitute a battery even if
it does not cause injury, and could not reasonably be
expected to cause injury. A defendant who emphatically pokes
the plaintiff in the chest with his index finger to
emphasize a point may be culpable for battery (although the
damages award that results may well be nominal). A defendant
who spits on a plaintiff, even though there is little chance
that the spitting will cause any injury other than to the
plaintiff's dignity, has committed a battery.
Assault and
battery has a 6 month custodial sentence and a £5000 fine at
Magistrates Court.
We hope that Leighton
Hospital will now reveal the names of the people who
committed these crimes as up to now they have been
protecting these criminals by failing to supply their names.
The ruling is significant as Leighton Hospital give
suppositories all
the time without consent so now people can sue them for this
and the doctors can be struck off. Many patients have
complained to us that they had there underwear removed while
they were sedated totally without their consent. The
hospital just don't understand the effects this has on
people and they are committing criminal acts by doing it
Experts Opinion
1. We sent Steve Bolsin BSc, MB BS, FRCA, FANZCA, MRACMA,
MHSM, DLitt (Hon)
Director of Perioperative Medicine, Anaesthesia & Pain
Management
The Geelong Hospital Geelong Victoria 3220 the notes and
asked for his comments which are
I have reviewed the notes that you have sent and certainly
there is evidence of a large overdose of lignocaine and an
inappropriately high dose of midazolam in the first
instance. However there are other more systemic issues
relating to the planning and anaesthesia for such an
operation. For example it might have been safer to undertake
the procedure on a patient weighting 135 Kg under general
anaesthesia to anticipate and prevent some of the potential
problems that arose during the procedure. Who undertook the
anaesthetic assessment for the patient? What type of block
was used for the surgery? What factors led to the operation
taking 2 hours? Why was the atropine given? (Presumably for
bradycardia). What was the cause of the bradycardia? Why did
the surgeon proceed with any operating while the patient was
in pain? This would imply withdrawal of consent for the
operation at that time and under those circumstances and may
be an assault.
The specific answers to your questions are: Yes it is far too much midazolam in one dose and is evidence
of lack of experience with the drug and the technique of
sedation.
The local could drop the heart rate but if the patient could
not breath then there may be more significant reasons such
as hypoxia followed by bradycardia.
The local dosage is a large overdose and inappropriate in
the circumstances.
I can not see the correction in my copy but if there has
been an alteration this is a very significant piece of
information in itself. You need to find out who altered the
chart and for what reason? If the bradycardia was due to
hypoxia the saturations must have fallen. If there was no
fall in saturations then the bradycardia was due to the
local anaesthetic overdose and is still very significant.
Yes the operation should be pain free.
Hyperthermia for long operations can be easily prevented by
warming blankets. these usually blow hot air over the
patient and should have been used for any operation taking
more than 20-30 mins.
I hope this brief assessment helps you.
Steve
Effects of the operation
An open letter to nurses and doctors
Special note here the patient express her personnel
feeling of what happened during an operation she was sedated
for some of the experience with a drug known to give sexual
daydreams.
I went into Leighton hospital for a simple hernia operation as a day
case and before the operation I told the nurse I didn’t want
my knickers removed. She said as I was 21st they were not in
the way and that was fine I also told her I didn’t want a
suppository. I was taken into the anaesthetic room and given
a massive dose of Midazolam 10mg all in one go according to
my medical records.
I then started having a terrifying dream of being gang raped
I was in a room full of people and they were removing my
knickers in the most dirty, vile filthy and perverted way I
feared for my life. I was unable to stop them doing these
vile things to me and I was totally humiliated being
stripped in public in this way it was the most terrifying
experience of my life.
Midazolam is know to enhance sexual
feeling and lots of cases of people having these
feeling that's why it popular as a date rape drug. My knickers were removed for none
medical reasons they claim so they wouldn’t get stained. Any
women would prefer to loose a 50p pair of knickers instead
of being forcible striped by complete strangers. I don’t
know if it was done so people could look at my private parts
in order to get sexual pleasure or what. As it’s a criminal
offence of Assault and Battery which can have a 6 months
custodial sentence I wouldn’t think anyone would do it
without they got pleasure out of it. To ask a women while
awake to remove her own knickers is one thing but to
forcibly strip someone is a totally different thing As I was coming around
from the operation I was awake when a nurse lifted my legs
and buggered me.
Both the things were done totally without my consent and
expressly against my wishes I don’t care how good a reason
you had you did it totally without consent and for that
reason its sexual assault.
It has now been nearly 2 years since this happened and I
still wake in the night from horrendous nightmares screaming
and trying to cover my self from the sexual assault my heart
rate goes through the roof and I cant breath. My life
has changed I am dirty and can never be clean again I have
been sexually abused just the same as if I had been raped
but its worse than that as I was helpless and had no way of
stopping the attack, I couldn’t even fight back. I cant
have any sort of sexual relations as I am unclean and cant
stand the thought of anyone touching me. I have been
buggered and deeply humiliated
without my consent has taken place and once again I was
unable to stop this happening to me.
What makes this worse is the hospital refuse to sack this
woman or name her so she can be brought to justice. She has
no excuse for what she did its her job to ensure she obtains
consent before she touches anyone and simply asking if its
ok and explaining what she wanted to do is all it took but
she didn’t do any of these things just simply buggered me.
No decant caring nurse would do this terrible
thing without first obtaining consent.
In the last 2 years I have lost over 11st in weight due to
this incident. If I go out and see a group of people it can
bring on panic attacks were I think they are going to strip
me again my heart races and I cant get my breath. The
attacks can happen watching television if there is anything
similar to what happened to me. My life is a total mess I am
depressed and often go into a world of my own for a week at
a time. I cant talk about what happened without getting
flash backs.
The hospitals attitude is once you give consent to an
operation they can do what the fucking hell they like to
you. For senior management to refuse to give the names of
the perverts that did this is unbelievable. The senior
management at the hospital refuse to answer any emails and
have not bother to even apologise for the sexual assault
they claim it was all done above board but if you bugger
someone and remove their underwear without consent there is
no grey area its assault. The GMC have
ruled that these things were done without consent so there
is no doubt that in the eyes of the law a crime has been
committed but still the hospital refuse to name or
discipline the nurses who have done this to me.
I want all doctors and nurse to read this and I hope they
will then think before they do anything to a patient without
first obtaining consent they must remember that people are
not just pieces of meat but have feelings and fears and are
very vulnerable. Maybe reading this they will understand
what effect their actions can have on someone. To them
removing underwear is nothing but to many this has the
effects that I have described. Many modern women might not
mind but there are thousands who feel like I do.
I noticed
my time in hospital that most don’t ask consent or explain
what they intend to do they think they are gods better than
the rest of us and can abuse patients and get away with it.
I believe that most of the violent attacks on staff are
because they don’t explain what they are doing and don’t
seek consent. It take a second to say I want to take some
blood is that ok.
I do accept that the
whole incident was done for all the right reasons and
nothing untoward happened but this doesn't make any
difference to what I felt and what I still feel a lot of the
feeling I believe are enhanced by the drug Midazolam that
they used and it show they have considered the side effects
of this drug.
Midazolam can lead to the patient experiencing daydreams
with a sexual content.
These are the GMC Rules for good medical practices for surgeons and every hospital should use these as their standards. If they
don't you can complain to the GMC
Here
These rules apply to minor operation done on a day patient as
well.
Consent
Intimate
Examinations
December 2001
The GMC regularly receives complaints from patients who feel that
doctors have behaved inappropriately during an intimate examination.
Intimate examinations, that is examinations of the breasts,
genitalia or rectum, can be stressful and embarrassing for patients.
When conducting intimate examinations you should:
Explain to the patient why an examination is necessary and
give the patient an opportunity to ask questions.
Explain what the examination will involve, in a way the
patient can understand, so that the patient has a clear idea of
what to expect, including any potential pain or discomfort
(paragraph 13 of our booklet
Seeking patients’ consent gives further guidance on
presenting information to patients).
Obtain the patient’s permission before the examination and
be prepared to discontinue the examination if the patient asks
you to. You should record that permission has been obtained.
Keep discussion relevant and avoid unnecessary personal
comments.
Offer a chaperon or invite the patient (in advance if
possible) to have a relative or friend present. If the patient
does not want a chaperon, you should record that the offer was
made and declined. If a chaperon is present, you should record
that fact and make a note of the chaperon’s identity. If for
justifiable practical reasons you cannot offer a chaperon, you
should explain that to the patient and, if possible, offer to
delay the examination to a later date. You should record the
discussion and its outcome.
Give the patient privacy to undress and dress and use drapes
to maintain the patient’s dignity. Do not assist the patient in
removing clothing unless you have clarified with them that your
assistance is required.
Anaesthetised patients
You must obtain consent prior to anaesthetisation, usually in
writing, for the intimate examination of anaesthetised patients. If
you are supervising students you should ensure that valid consent
has been obtained before they carry out any intimate examination
under anaesthesia.
You may find some hospitals don't get the proper consent and if
for instance they were to give you pain relief by way of a
suppository while you are under sedation if they do they must get
your permission in writing before you are sedated or the doctor may
be struck off for assault. A lot of Hospitals use
Midazolam (versed) for sedation
during minor operation like a hernia and by the rules they must tell
you the risks.
One of the risks is it can make you forget which you
may think is a good thing but some people don't want to forget. You
may be given a pain relief Voltkol which is given as a
suppository if they haven't told you about this and obtained your
permission in writing as per the above GMC rules then you can
complain to the GMC or look for compensation for sexual assault. The
problem is because of the Midazolam you may not know they did this
you would have to apply for your medical records to see. You don't
need this pain relief you can have tablets and according to the
rules they must explain this to you and give you the chance to opt
out.
Health watchdog finds that failings at the Mid Cheshire Hospitals
NHS Trust led to unacceptable levels of care for older patients
Published: January 24th 2006 Serious lapses in the care of older
people at Leighton Hospital have been identified in an investigation
report published today (Tuesday) by the independent healthcare
regulator the Healthcare Commission. The investigation followed the
conviction in 2004 of Ward Sister Barbara Salisbury on two counts of
attempted murder.
The conviction related to incidents that occurred at Leighton
Hospital in 2002 and involved the inappropriate administration of
diamorphine, a powerful opiate analgesic, to patients. The aim of
the investigation was to look at whether there were failings in
systems to protect patients in the trust in 2002, and to assess
whether these failings were still a problem. The investigation found
that the trust failed to meet adequate standards of care.
This, together with poor leadership and management, staff shortages
and a lack of learning from complaints, resulted in the safety of
patients being compromised. Patients were often not assisted to take
their medication or helped with eating and drinking. The Commission
found that the general lack of attention by staff sometimes
prevented patients from getting to the bathroom or using the bedpan
in time, adversely affecting their dignity, morale and health.
Healthcare assistants reported having no time to shave patients or
answer buzzers, and there were numerous examples of drug rounds
being late and tablets being left on tables out of reach of
patients. Following the conviction of Barbara Salisbury, many nurses
and some families reported serious misgivings that patients were not
receiving adequate pain relief. Marcia Fry, Head of Operational
Development at the Healthcare Commission, said: “There is no excuse
that allows for the care and dignity of patients to be compromised
in this way. “This report has highlighted serious problems, some of
which go right up to the most senior level at the trust.
We are pleased that the trust has already taken some urgent action
to improve the service for patients. It must continue on this path
and make every effort to implement all of the recommendations in
this report. It must do everything in its power to build a service
that staff, patients and their families can rely upon. “As
performance manager and commissioner of services of the trust, the
local strategic health authority and primary care trust must share
responsibility and work with the trust to improve the situation.
“The Healthcare Commission will keep a close watch on the trust over
the coming months to make sure that the necessary improvements are
made.” In order to address the concerns identified in the
investigation the Healthcare Commission has made the following
urgent recommendations:
* Recruit additional frontline nursing staff to provide an
acceptable and safe standard of care
* Improve governance and management of the medical directorate
* Investigate and address the cause of poor clinical outcomes in the
medical directorate, including apparently higher than average
mortality rates in recent years
* Review management and accountability arrangements in the trust In
addition, the trust must also:
* give greater priority to the care of older patients in line
with the national service framework for older people
* provide care that puts the needs of patients first and treats them
with dignity and respect
* review its arrangement for providing patients with
appropriate pain relief
* take action to address poor care when it is identified
through complaints and/or reporting
* develop action plans in response to serious complaints and ensure
that they are implemented and monitored Mid Cheshire Hospitals NHS
Trust have developed a detailed action plan to address the
recommendations in the report.
A number of these actions have already been put in place including a
high level review of the trust’s management arrangements. The trust
is reviewing its risk assurance framework; they are also reviewing
arrangements for governance and management particularly in the
medical directorate. In addition to this, the trust, which is under
the leadership of a new acting chief executive, has recruited 44 new
nursing staff, and introduced a new approach to handling and
learning from complaints. An audit of the care of older people has
been launched. Cheshire and Merseyside Strategic Health Authority
and the Healthcare Commission regional team will closely monitor
progress made against the action plan.
Nurse gets five years for seeking to kill two
patients but was
she innocent?
Nurse gets five years for seeking to kill two
patients
Ward sister weeps at verdicts after trial that heard
of her ruthless desire to free beds by causing
elderly to die
Helen Carter
Saturday June 19, 2004
The Guardian
A senior ward sister was convicted yesterday of
attempting to murder two elderly patients under her
care because she was motivated by a ruthless desire
to free up beds at a hospital which was in the
throes of a bedblocking crisis.
Barbara Salisbury crossed the line between humane
nursing and callous dispatch of patients at Leighton
hospital in Crewe by administering diamorphine or
lying them on their back so they would drown in
their own secretions. She was jailed for five years
after being found guilty at Chester crown court of
the attempted murders of May Taylor, 88, and Frank
Owen, 92, in March 2002.
Article continues
Salisbury, 47, from Pontybodkin, north Wales, wept
as the guilty verdicts were read out. Sentencing
her, Mr Justice Pitchford said: "Your duty and your
trust was one of care towards your patients, and
under the direction of the doctors, the respect for
and preservation of human life. The jury has found
that in the case of two elderly patients who were
nearing their end, you broke that duty and abused
your trust by attempting to hasten death."
He added: "It is impossible for me to fathom what it
was to cause you to act as you did. You chose to
exercise control over life and death of patients
whose time had not quite come."
Salisbury had faced four attempted murder charges.
But she was cleared of any unlawful involvement in
the deaths of James Byrne, 76, and Reuben Thompson,
81.
Two years ago, the Cheshire hospital which serves a
community with a large number of elderly people, was
in the middle of a bedblocking crisis, which has
since eased. The court heard that when she arrived
back on the ward after six days off sick, she saw Mr
Owen, who had been a patient for three months, and
asked: "What's he still doing here?"
The prosecution said she had been constantly
pressing for him to be discharged to a nursing home,
despite Mr Owen needing a drip. She told her
colleagues to lie him on his back "so his lungs will
fill with fluid and he will die".
Despite colleagues telling her that Mr Owen was not
in pain, she gave him two injections of diamorphine.
The former mechanic died five minutes after she
finished her shift. One witness described her
actions as "callous and unprofessional". Later, she
was asked if his death was peaceful. She replied:
"Yes, thanks to me."
Salisbury had lied to doctors to ensure Mrs Taylor,
a widow, was given excessive doses of diamorphine.
When challenged, Salisbury had replied: "Why prolong
the inevitable?"
She had been accused of telling James Byrne, who had
suffered a minor stroke: "Give in, it's time to go,"
as she gave him diamorphine.
When she appeared in the witness box, Salisbury
repeatedly denied hastening patients' deaths, but
admitted using the phrase "It's OK to go now" to
those close to death, in an effort to be soothing.
The prosecution claimed Salisbury had arrogated to
herself the right to decide when patients should die
and attempted by her actions to shorten what
remained of their lives. But she said: "I have
probably said, 'It's OK for you to go now.' It's a
term I often used to use in intensive care, meaning
it's OK, you can leave this life," she told the
jury. "I said it in a gentle way to let them know
there was somebody there." She could not remember
any of the four patients.
Unpopular
Salisbury was said to have been unpopular among her
colleagues on the ward because of her brusque
manner. Many of the nurses were traumatised by what
they witnessed, while others were bullied into
obeying her orders. Following the death of Mrs
Taylor, nurses Katherine Darby and Alexandra McNally
were so appalled by her treatment at the hands of
Salisbury that they complained to their managers.
There were other incidents involving elderly people.
Nurse Annie Denson said that on Christmas Day 2001,
Lila Hillyer, 86, was nearing death. She had left
her on her side aided by an oxygen mask so she might
survive until relatives could see her. Then
Salisbury came into the side room and said: "Lose
the oxygen and lie her flat." The nurse ignored the
instruction and the patient survived two more days.
Salisbury's barrister, Peter Birkett, said in
mitigation that she had no criminal record and
suffered from depression, for which she was treated
in hospital from August 2002 to July 2003.
Salisbury, a mother of two, had been a nurse for
most of her working life. Born in Liverpool, she
began training in 1975 while in the RAF. She went on
to qualify as a state enrolled nurse and a
registered general nurse and worked at hospitals in
Peterborough and King's Lynn, principally in
intensive care. In 1993, she moved to Leighton
hospital. She had risen to the rank of Grade E staff
nurse and three years later she was promoted to a
Grade F ward sister.
She worked on Ward 5, a general medical ward with a
number of geriatrics, until 2000, when she
transferred to Ward 4. The following year, the
trust's chief executive, Simon Yates, presented her
with a Learning to Be a Leader award.
"She had a pretty good reputation with the
management," said a source at the hospital. "They
looked upon her as being efficient. But the people
who worked with her had no time for her at all. They
certainly didn't like her attitude and she upset and
offended an awful lot of people."
For more than a year, a team of detectives from
Cheshire police were based at the hospital as part
of a lengthy investigation led by Detective Chief
Inspector Adrian Wright. Salisbury was eventually
charged with the attempted murders in June 2003. The
inquiry team examined 20 deaths of elderly patients
at the hospital over a five-year period. A hotline
set up for concerned relatives received more than
100 calls in its first few weeks.
In a statement, the Cheshire and Merseyside
Strategic Health Authority paid tribute to the
whistleblowers. "We are grateful to the hospital
staff who first raised their concerns with the trust
for bringing the matter to the attention of the
police," it said. "We have agreed with the trust
that the SHA will commission an independent
investigation to look into the issues surrounding
this case."
A statement from Salisbury's husband Derek said: "My
wife is a devoted nurse, who has dedicated herself
to the care of the sick. Always she has put the
interests of patients first. We do not accept this
jury's verdict. We know her to be innocent of any
crime. This is a tragic day for her, for us her
family, and for the nursing profession."
Full report of the investigation and how it was conducted